MCL Tears – The Road to Recovery after Medial Knee Injury
People who participate in high speed, or multidirectional sports will be likely at some stage to experience an injury to the leg joints, like twisted ankles, or a pulled muscle at the hip. But there is something about knee injuries that make soccer players, skiiers, frisbee players, rugby players and even rollerskaters wince.
Within the knee there are a group of large ligaments that work to provide stability to the joint at all angles. We can thank their thick collagen make-up for this structural strength. But ligaments also provide a mental support to the joint, known as proprioception. Small fibers in the ligament send messages to the brain when they are being stretched and loaded, preparing the brain for this stress or using it to tell the brain to change direction soon to avoid injury. But what happens when this fails? Or when the load is just too excessive or comes on too quick?
The ligament (and possibly other structures) pay the price. The Medial Collateral Ligament, or MCL is a structure we see commonly injured within the knee joint, closely associated with ACL tears, and meniscal (or cartilage) injuries. To understand how this ligament ends up being commonly injured in multidirectional sports, it is super helpful to be aware of where it is situated and how it works.
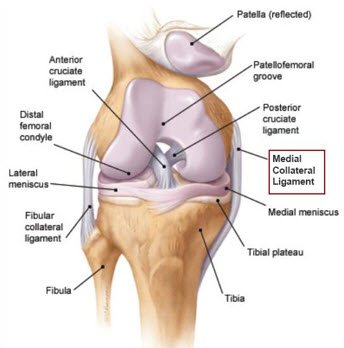
The MCL is a large ligament that is about 1.5cm wide and on average, measures an average 11cm (Phisitkul et al., 2006). The ligament is made up of 2 portions, the superficial and deep MCL. The superficial part of the ligament has been shown to limit valgus and external rotation forces. This means preventing the knee from buckling inwards and preventing the shin bone, or tibia, from rotating out at extreme angles. In this way we can say that the MCL helps protect other structures within the knee such as the menisci and ACL/PCL complex. The deep portion of the MCL helps stabilise the hamstring tendon as it attaches into the back and inner portion of the knee.
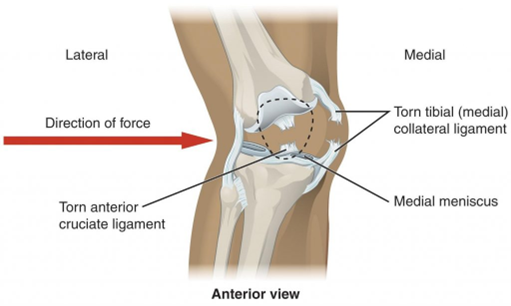
In the image above, you can see the stress is coming from the outer aspect of the knee, and this impact causes a large force through the MCL, frequently causing injury.
This type of impact can occur during contact sports, like a kick or tackle to the outer knee in soccer or wrestling, or can occur in a non-contact scenario, where in changing direction or squatting on one leg a similar position occurs and is worsened by the body’s weight acting down on the knee. This is seen in skiing, ice hockey, rugby, or in non-sporting injuries such as slipping on wet floors or uneven ground. Non-contact MCL injuries are typically more common than contact MCL injuries.
As far as knee injuries go, the MCL can be easily assessed by a physiotherapist or sports doctor and immediate MRI or x-ray referral is not always required. This can be organised depending on the extent of the injury and to rule out other injuries such as ACL or menisci tears. However in the case on MCL injuries alone, it is rare that an MRI or ultrasound scan will affect how your physio manages the injury.
So how bad is my injury? Your physio will do some tests to define how badly they think the ligament has been damaged. In terms of classifying the injury – ligament tears are usually graded based on the percentage of fibres damaged.
Brukner and Khan’s Clinical Sports Medicine Guidelines guide us on this classification. They are graded from 1-3 and you can see a rough guide on how long it takes for these injuries to heal.
Grade I MCL Sprain Partial fibre disruption 0-2 weeks
Grade II MCL Sprain ~ 50% fibre disruption 2-6 weeks
Grade III MCL Sprain Full rupture 6-12 weeks
Once your physio has diagnosed the MCL sprain, they can formulate a course of treatment. Following guidance from a 2021 study (Naqvi et al.), the rehabilitation pathway most commonly followed for MCL sprains is conservative. This comprises the POLICE protocol", Protect – stay way from harming the ligament further, Optimally Load – Some injuries can tolerate some weight bearing and may not require complete rest from taking body weight, Ice, Compression and Elevation. The use of knee bracing such as DonJoy braces can be helpful for those who are injuryed and do not tolerate load well or in which there is a higher degree of laxity on testing.
For Grade III injuries (full rupture), some more thought must be put into management. This is for a few reasons. Grade III MCL injuries are commonly accompanied by other knee structure damage, such as ACL or menisci. Surgery is commonly discussed if there are multiple damages to knee structures, but some people may still opt for conservative management even in these cases. The age and activity level of the individual should be considered, as similar to ACL and meniscal injuries, a successful return to sport and long term knee health can be influenced by a surgical approach. Lastly, larger scale MCL tears usually lead to laxity on testing of the inner knee structures, if there is medial instability when the knee is fully extended, then a surgical approach will likely be discussed, as this can impair function in even inactive individuals, and should be avoided to maintain a decent quality of life.
In certain sports such as rugby and AFL arguments have been made in favour of wearing protective knee braces to prevent healthy knees from sustaining MCL injuries. This was investigated in 2010, by gathering data on studies who had trialled these braces on American Football Players. Out of 3 studies, there was a reduction in MCL injuries sustained that year, and the general conclusion was that the braces has provided some protection. However, 2 of the 3 studies actually saw in increase in MCL injuries during the American Football season. From this information, we would not conclude that the bracing caused this influx in MCL injuries but can safely conclude that they do not provide an effective barrier against MCL tears. It is also important to note that there is simply not enough studies for or against the use of these braces to guide us on their use, so from an injury prevention stand-point, we suggest scrapping the use of supports and braces and investing some time into a decent lower leg strength program.
What can I do to prevent a MCL injury?
This can be provided even for those who have no history of knee injury, and is highly recommended for those who play multidirectional sports, or those who or move or compete on unstable surfaces. The main muscle groups we will pay attention to are the quads, hamstrings, and control of the hip musculature. A muscle group frequently forgotten in lower leg strength and knee injury management are the groin muscles. They provide stability of the inner thigh, and their attachment, along with 2 hamstring tendons, is congruent with fibres of the MCL. Groin strength is imperative for MCL protection in the sports of skating, skiing and ice hockey. The hip stabilisers, or glute muscles prevent knee valgus also by working hard to externally rotate the thigh bone, or femur. Therefore if the knee is in a precarious position during a direction change or rapid deceleration during a game, MCL or ACL injuries can occur if the lateral hip doesn’t kick in fast enough to act against these high forces. See our ACL blog for more information on these common positions of injury for knee ligaments.
So in conclusion, MCL injuries are common in the world of sports, and can be managed without the need for surgery in most cases. As with other lower leg injuries, we recommend the best way to prevent these from slowing you down during the sporting season is maintaining good muscle strength and practicing drills to improve your mechanics.
References
Phisitkul P, James SL, Wolf BR, Amendola A. MCL injuries of the knee: current concepts review. Iowa Orthop J. 2006;26:77-90.
Naqvi U, Sherman Al. Medial Collateral Ligament Knee Injuries. [Updated 2021 Jul 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431095/
Salata MJ, Gibbs AE, Sekiya JK. The effectiveness of prophylactic knee bracing in american football: a systematic review. Sports Health. 2010 Sep;2(5):375-9. doi: 10.1177/1941738110378986. PMID: 23015962; PMCID: PMC3445064.
Written by
Angela Crowley
M.R.S Physio