Lateral Hip Pain: Bursitis vs Tendinopathy & Physiotherapy
Lateral hip pain? Bursitis v Tendonopathy
Lateral hip pain is a common concern and it occurs mostly in runners, avid walkers, and young athletes. Pain specifically on the side of the hip can be particularly debilitating, especially when it starts to affect your sleep and activities of everyday life.
Your physio must gather a full history including activity levels, or any relevant changes to this, working position and past medical history including the lower back and lower limb injuries. Some physio tests can be done to rule out a pathology of the lower back back or hip capsule.
Lateral hip pain is characterised by tenderness around the bony outer part of the hip, called the Greater Trochanter (GT), and pain in loading of the muscles that attach to the GT. A population which are commonly affected by lateral hip pain are women over the age of 40 due to the angle of which the femur orientates with the pelvis, and often weaker gluteal muscles than their male counterparts.
Your hip pain may be aggravated by:
prolonged standing,
walking,
running,
sleeping on the affected side
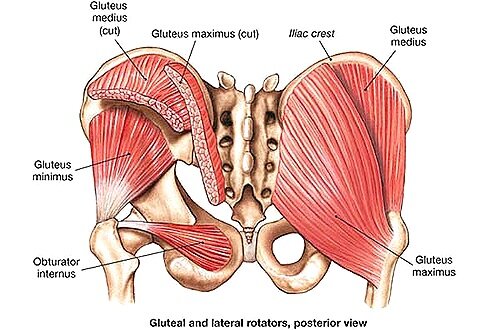
Muscles most linked with pathology of the lateral hip are both the Gluteus Medius and Gluteus Minimus, in particular, their tendons. The image above shows the tendons of these muscles attaching onto the GT, which is the tender point often mentioned in the subjective exam. This pathology is called Gluteal Tendonopathy. Its examination and treatment is similar, relatively, to any other tendonopathy in the body. For example, the Achilles Tendon, which is commonly affected by tendonopathy reduces its ability to take load over time. This gradually worsens as the tendon starts to change at a molecular level in an attempt to adapt to your activity workload. The hip acts no differently, and its tendons respond similarly when adapting to changes in load.
With tendonopathies, pain occurs at the beginning of exercise, and the following morning. Athlete’s can usually “push-through” pain as they warm up, but pain returns once they cool down.
Researchers have formulated a reliable rehab protocol that is found to be extremely successful in treating tendon pathologies. Visit our Achilles Tendon blog here to review the protocol. Regarding the hip, physio’s must be specific in which tendon is causing the problem. Testing certain hip movements, and finding weakness or a painful response helps us identify the muscle and tendon at fault causing the symptoms.
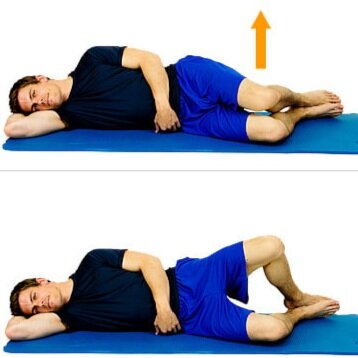
Below are some movements that your physio may use to identify which tendon is at fault.
Hip abduction as shown in the picture to the right when done properly, will cause Gluteus Medius to activate.

Clams, or hip external rotation, picture shown to the right, will cause external rotators such as the gemelli to work, but mostly, Piriformis.
Using this information and identifying the pathological tendon, we can provide you with an individualised exercise rehab program. Depending on the activities or sports you play it may involve different exercises gradually progressing from isometric to eccentric to sports specific exercises, thus improving the loading capacity of the affected tendons.
Brukner and Khan (Clinical Sports Medicine, 5th Edition) discuss how certain positions of the lateral hip can cause compressive loads to accumulate in this area. This can occur from static postures, such as standing “hanging on one hip” into adduction (picture below), sitting with knees crossed, or completing functional tasks with excessive lateral hip tilt or shift. This is called a Trendelenberg sign (Picture b)) and occurs when the outter hip muscles do not pull the hip into abduction while standing, walking or running, or during gym activities.

a) Standing hanging on one hip, causing strain on lateral hip muscles.
b) Test for the Trendelenburg Sign
A positive Trendelenburg sign usually indicates weakness weakness in the hip abductor muscles consisting of the gluteus medius and gluteus minimus.
A positive sign is when the pelvis drops on the opposite side while on a single leg stance on the affected side.

But what if the tendon isn’t the issue? What if on testing, there is pain provocation, but no weakness of the muscle being tested. What if a tendon doesn’t respond to tendonopathy protocol with progressive loading? The differential diagnosis could be the underlying bursa.
Differential diagnosis Hip bursitis
Within the body, we have small fuid-filled sacs that are called Bursae. They act as mini air-bags that can inflate and swell when they get irritated. They are found between two tendons, or between tendon and bone. Irritation of the Bursae is called Bursitis. It occurs commonly in the hip, knee, Achilles, and shoulder. These joints are also known to be popular with tendinous issues. We can safely say that tendon pathologies can go hand in hand with Bursitis. This is because the Bursae inflating can be the body’s way of letting us know there is an irritation and a possible abberant loading or mechanical issue within the joint.
Bursitis can occur without any tendon changes, and the subjective history is usually different to that of a true tendonopathy.
What are the symptoms of Bursitis?
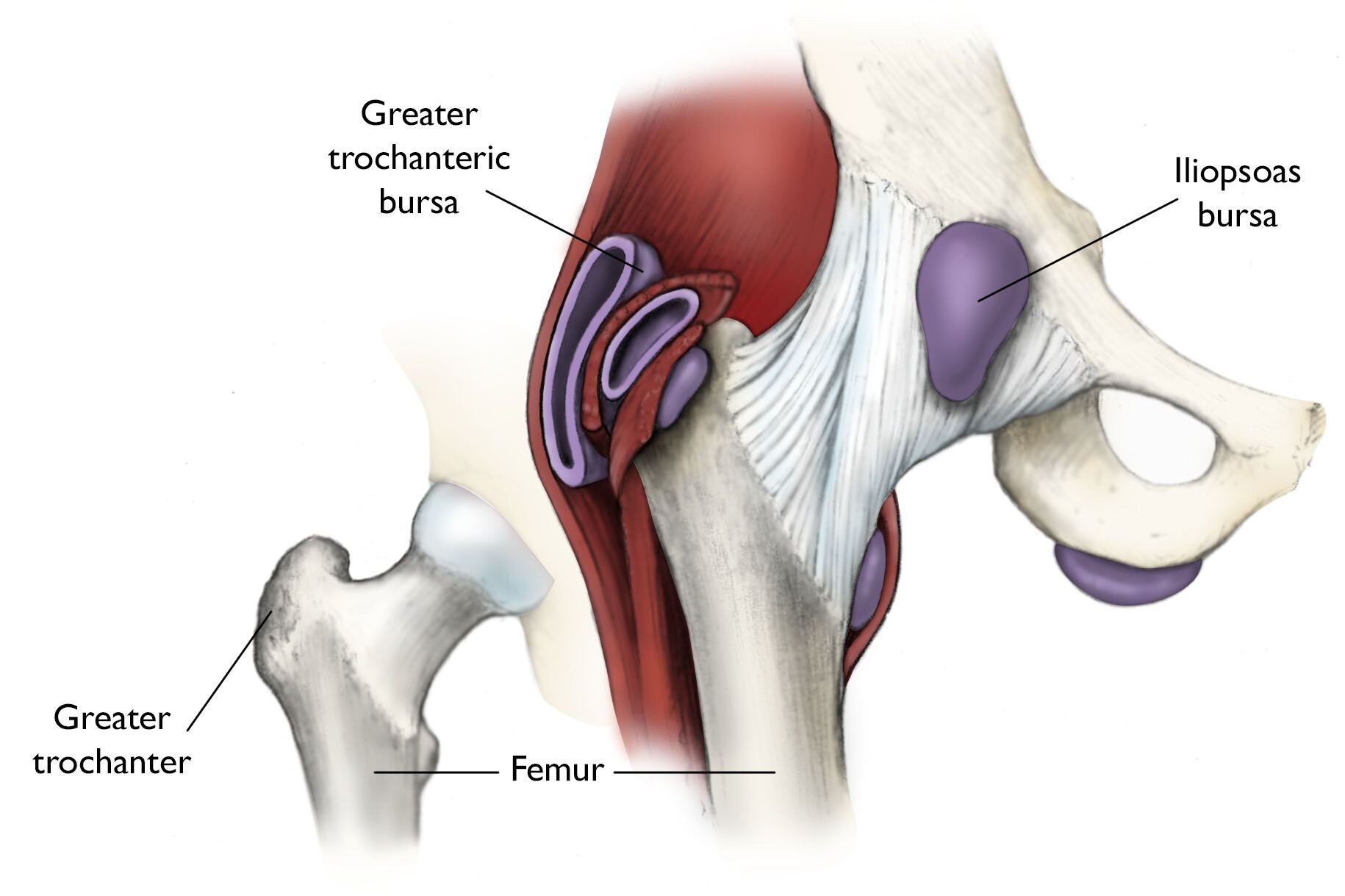
Bursitis of the lateral hip (picture below) is characterised by localised pain on the side of the hip, like that of a tendonitis, but can be accompanied by soft swelling over the painful area.
Bursitis patients usually describe pain similar to those of Tendonopathies, but the pain usually worsens with activity, as the frictions caused by the tendons moving over each other or their bony attachments cause the Bursa to increase in size, and causes more pain with increased movement.
Bursitis is inflammatory in nature so will improve with rest, gentle stretching and icing protocol. It also is known to respond well to anti-inflammatory medications such as Ibuprofen, which is widely prescribed.
It is important to identify if there is indeed a tendinous issue causing the bursitis, as this must be treated accordingly as mentioned above. In theory, if the bursa is the only issue found on both subjective and objective assessment, then reducing inflammation of the bursa, gentle stretching of the fibres creating the irritation (gluteus medius, minimus and TFL) and reducing the aggravating activity so that movement is pain free, for example walking, running, squatting, high intensity interval training classes etc.
Progressive strengthening to support the structures surrounding the bursa should be undertaken, including general hip stability work, balance retraining, alignment and co-ordination exercises.
Functional activities should be looked at in detail to ensure Trendelenberg sign, lower back abnormailities or weakness, or knee or ankle dynamics are not causing knock-on patterns at the hip. It is important to remember that Bursitis is usually a warning sign that something else within the lower limb isn’t working correctly, so care should be taken to ensure this is identified to reduce recurrence of Bursitis.
Written by:
Angela Crowley
M.R.S Physio Auckland
Editted by:
Jenny Chen
M.R.S Physio Auckland