Thoracic Spine: Unlocking the Cranky Upper Back
A Physiotherapist’s take on the treating the mid spine.
Have you ever injured your neck, and found it difficult to move your head side to side? Or strained your lower back in the gym and found bending over to tie your shoelaces was difficult? These are really common injuries, and happen so often as we see the neck and lower back as super mobile areas of the body. But what do you do when you have a stiff and cranky upper back? The thoracic spine can be as easily injured as its neighbours above and below him, but the vast majority of upper back pain stems from prolonged periods of idleness; for example, sitting or standing. Let’s try to unearth the reasons why the thoracic spine can cause such grumbly and irritating pain in many populations.
To begin, we must understand the anatomy of the upper back, or Thoracic Spine as it is more officially titled. This section of the spine consists of 12 vertebrae which look similar to those of the lumbar or cervical spine, except for an obvious size difference and in addition, on each transverse process (or each wing) of every thoracic bone there lies small surfaces which allow a rib to connect on each side.
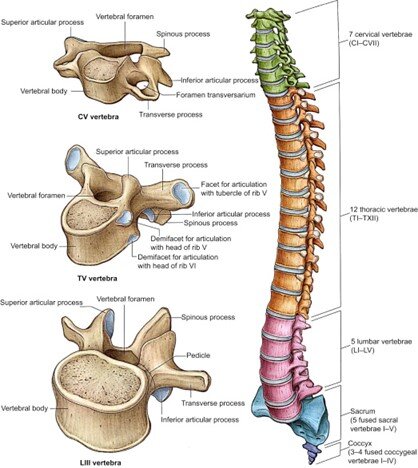
Ribs are connected together by cartilage at the sternum, or breastbone, and have muscles called intercostals in the spaces in between them that assist in expanding and contracting the ribs during breathing.
The Thoracic spine naturally sits in a curved position called a Kyphosis. A certain degree of kyphosis is normal to have, but some people suffer from congenital issues or sustain injuries in later life that cause a greater degree of kyphosis. It is also known to present more significantly in women, especially after the age of 40, and can be accompanied with osteoporosis. (Lam, J.C 2021)
An exaggerated thoracic kyphosis can occur from postural positions, for example, sitting in an unsupported chair or driving for long periods in a deepened car-seat. This does not mean the individual has changed the anatomy of their thoracic spine and created a long term worsening of their kyphosis, but it has the capacity to change the length and strength of the musculature around the ribcage and spine. These changes are found commonly on assessment of clients who have self-reported “postural pain” or note their pain occurs for prolonged sitting or standing.
A common complaint from those who work in sedentary positions, such as offices, is a stiff or achey pain in the upper back. This can be from prolonged sitting or standing – this shows that standing desks can be great but certainly are not the answer to everything. In this scenario, once the lumbar spine has been cleared and the client’s desk has been assessed to be made as ergonomic as possible, we can assume that reducing the large kyphotic stress on the thoracic spine and introducing ways to mobilise the spine into extension and rotation we can assist in reducing the client’s pain. Then strength work needs to be implemented to help maintain these changes so the person can work comfortably for longer periods before these symptoms kick in.
Our favourite exercises to improve thoracic mobility are:

(i) Extension over a foam roller or yoga ball
place the foam roller perpendicular to the spine (personally I like to work from the bottom to top of the spine).
Lace your fingers and place your hands behind your head to support the neck and gently arch backwards dropping the shoulder to the floor.
You can repeat this on the same segment for a few reps and move upwards to the next.

(ii)Threading needle thoracic rotations
Begin on your hands and knees, place our hands directly under the shoulders and knees directly under your hips.
Like the picture, lift the left hand and turn to the left. On the exhale thread the left hand under the right shoulder with your palm facing upwards.
On the inhale, unthread the left hand and repeat on the same side and perform on opposite side.
Let’s focus on some interesting presentations where the Thoracic spine could be a hidden cause of some or all of the client’s symptoms.
1. Shoulder pain in overhead movements
When patients present with shoulder pain that occurs in overhead movements, we must assess fully the rotator cuff complex, rule in or rule out active impingement from the subacromial space or a subdeltoid bursitis. As the shoulder is a complex joint, we just also assess the scapula and the relationship between it and the shoulder as the arm moves overhead. In some situations, you may have improved some symptoms in lower ranges or reduced active impingement, but the patient still complains of limitations in upper shoulder range that can be painful or just the feeling of blocking in certain exercises such as overhead press or pull-ups. You can try improving thoracic extension as an excessive kyphosis or stiffness in thoracic extension can create a mechanical block to gaining full shoulder flexion.
2. Cervical radiculopathy or excessive upper fibre trapezius tightness.
In prominent thoracic kyphosis postures, we often see a protraction of the chin, commonly referred to as “Tech Neck” these days.

This is often called “forward head posture” (figure A). In this position, sometimes we see a relative closing of the gap between joints in the lower neck. Irritation occurs most commonly between the C5, C6 an C7 vertebrae, and can easily irritate the nerve root adjacent to each, creating localised neck pain and in more severe cases weakness, numbness and pins and needles down the arm. These symptoms can also occur during neck rotation as it will further close in the lower neck joints. In circumstances where the symptoms have reached a plateau and we cannot fully regain cervical range of motion with chin retraction alone (figure B), then targeting thoracic extension and rotation can be the key to regaining full neck movement again.
It is important to note that this blog is highlighting the issues associated with extended periods of time in this position without periods of relief. Chin protraction or forward head posture is not “bad” in itself. As a rule, any position can cause pain if prolonged for too long a time with no rest in between.
Hopefully this blog provided you with some easy techniques and education around improving your thoracic spine mobility. Physios or clinicians, remember to focus on the upper back when treating sedentary individuals, to include it in your differential diagnosis in neck and shoulder injuries, and to always use in conjunction with education around prolonged working or studying postures for long periods of the day. And for anyone here researching their own upper back pain, remember to keep moving as much as you can throughout the day, and that the body was not designed to stay still for too long. You can have the perfect work station, but in the end, nothing is better than giving your body some well needed periodic mobility throughout the day.
Written by:
Angela Crowley, Physiotherapist
M.R.S Physio,
122 Remuera Road, Auckland.
References:
Lam JC, Mukhdomi T. Kyphosis. [Updated 2021 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK558945/